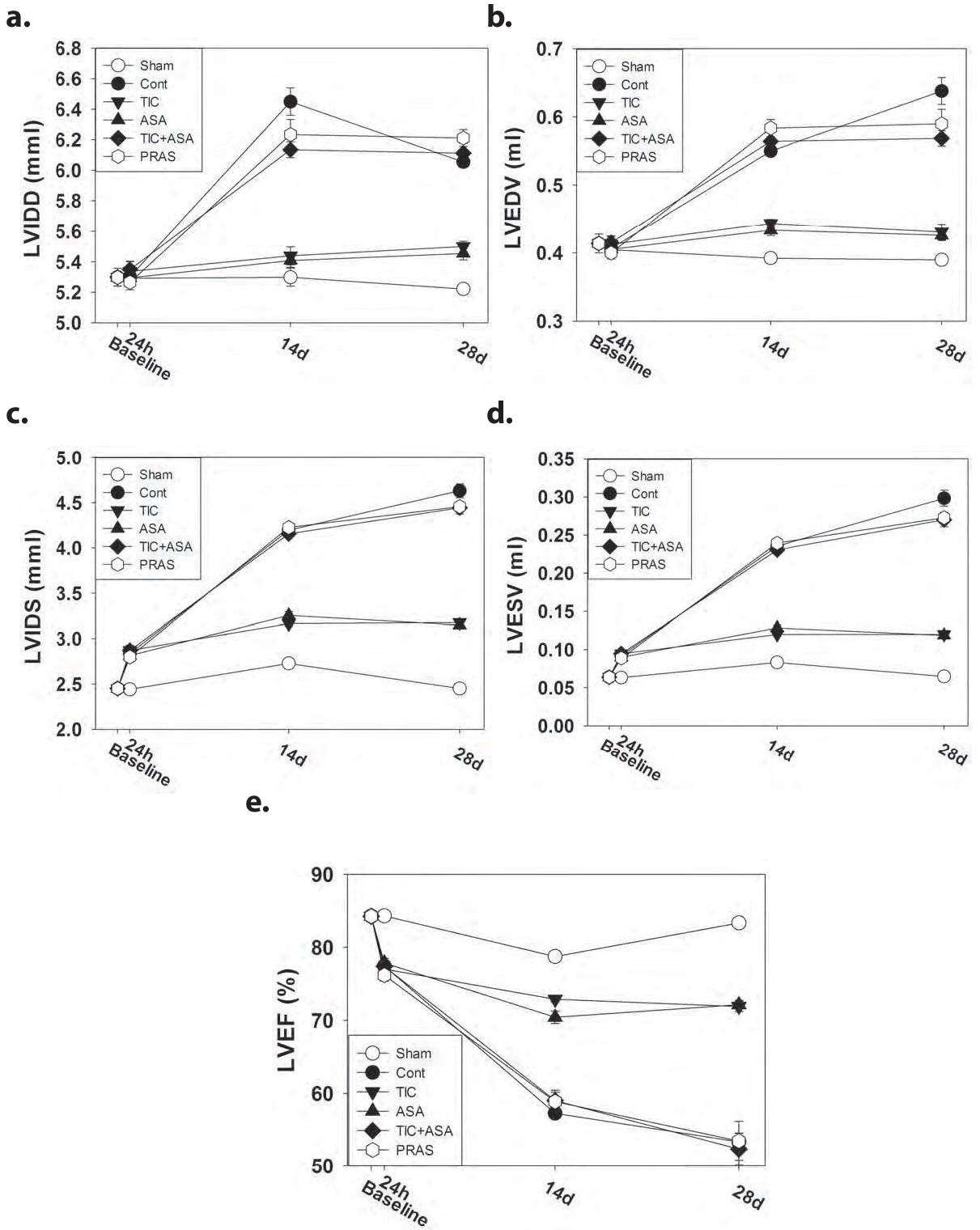
Fig. 2. Echocardiographic findings. A total of 8, 6, 8, 8, 7, and 7 animals were analyzed at day 28 after surgery for the Sham, Control, TIC, ASA, TIC+ASA and PRAS groups, respectively. a. Left ventricular internal diameter in diastole (LVIDD); b. Left ventricular end diastolic volume (LVEDV); c. Left ventricular internal diameter in systole (LVIDS); d. Left ventricular end systolic volume (LVESV); e. Left ventricular ejection fraction (LVEF). LVIDD were comparable among the groups at baseline and 24h after infarction (p=0.851). LVIDD increased in the Control group compared to the Sham group at 14d (p<0.001) and 28d (p<0.001) after infarction. At 14d and 28d, LVIDD was significantly smaller in the TIC (p<0.001 and p<0.001) and ASA (p<0.001 and p<0.001) groups than in the Control group. However, the increase in LVIDD over time was not affected by TIC+ASA (p=0.051 and p=0.999, respectively) or PRAS (p=0.455 and p=0.186, respectively). ASA- aspirin; Cont- control; PRAS- prasugrel; TIC- ticagrelor. No significant differences were seen in the LVEDV among the groups at baseline and at 24h after infarction (p=0.844). LVEDV significantly increased in the Control group compared to the Sham group at 14d and 28d (p<0.001 and p<0.001). The increase was attenuated by TIC (p<0.001 and p<0.001 vs. control) and ASA (p<0.001 and p<0.001 vs. control), but to a lesser extent with TIC+ASA (p=0.993 and p=0.022) and not at all with PRAS (p=0.160 and p=0.291). At 24h after infarction, LVIDS increased in all groups subjected to infarction, without differences among groups. However, at 14d and 28d the increase in LVIDS was attenuated in the TIC (p<0.001; p<0.001) and ASA (p<0.001; p<0.001) compared to the Control group, whereas TIC+ASA (p=1.00; p=0.287) and PRAS (p=1.00; p=0.391) had no effect. At 24h after infarction LVESV increased in all groups exposed to infarct compared to the Sham group, without significant differences among these five groups. However, at 14d and 28d the increase in LVESV was significantly attenuated in the TIC (p<0.001; p<0.001) and ASA (p<0.001; p<0.001), but not the TIC+ASA (p=0.999; p=0.068) and PRAS (p=1.00; p=0.143) groups. A decrease in LVEF was noticed 24h after infarction in all the five groups subjected to infarction compared to the Sham group, without significant differences among them. At 14d and 28d the decrease in LVEF was significantly attenuated in the TIC (p<0.001; p<0.001) and ASA (p<0.001; p<0.001), but not in the TIC+ASA (p=0.965; p=1.00) and PRAS (p=0.978; p=1.00).